Alexa Neynaber, ND | March 24, 2020
There is currently much discussion on Vitamin C and its role in healthcare during these unprecedented times. As Vitamin C and other nutrient-based therapies are within the toolkit and expertise of naturopathic medicine, the INM has provided an outlet to disseminate basic science information on this intervention. The Institute for Natural Medicine is a 501c(3) nonprofit organization with a mission to transform healthcare in America by increasing both public awareness of naturopathic medicine and access to naturopathic doctors for patients. From that perspective, the following information is not medical advice, rather, it is for educational purposes only.
Many believe that the healing capacity of vitamin C is an old wives’ tale or a marketing ploy to sell more orange juice. But the truth is that there is nearly a century of data that says otherwise.
In fact, vitamin C has been studied since the 1930s, and research has shown that it can improve quality of life for cancer patients, reduce incidence of infection, relieve fatigue, and more, while having limited negative side effects for most people.
If this sounds like fake news or dubious science, I encourage you to read on and assess the research for yourself.
Background
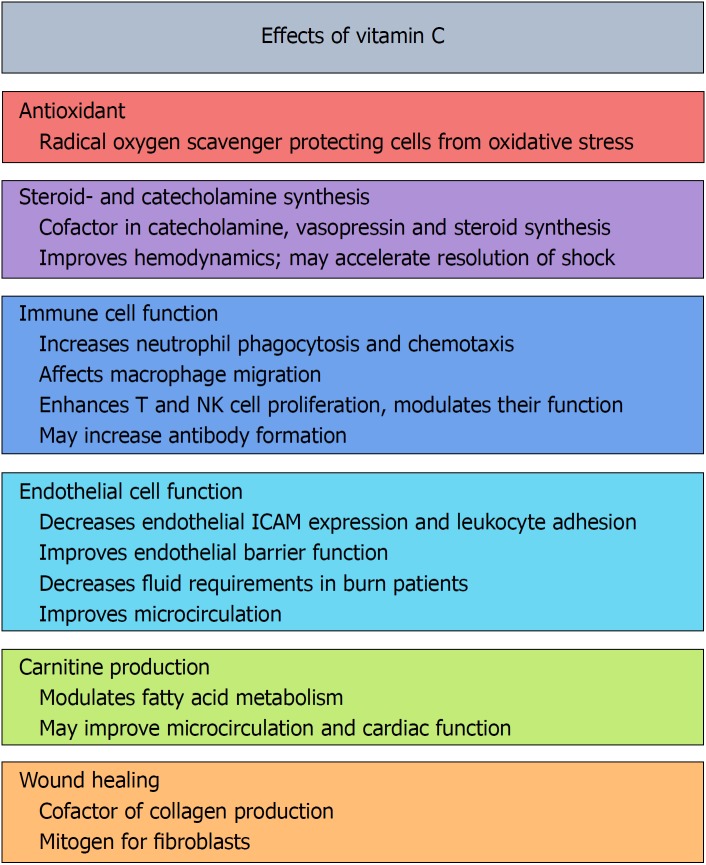
Vitamin C is a water-soluble vitamin and antioxidant. It is famous for collagen synthesis as it is necessary for cross-linking of collagen proteins, and it is needed for a multitude of functions in the body, such as in hormone synthesis and production of metabolic energy (Carr et al., 2017). It is an antioxidant because it can donate electrons to decrease reactive oxygen species (ROS) in the body. Antioxidants are important because they protect vital structures such as proteins, lipids, and DNA from oxidation and damage (Carr et al., 2017).
Vitamin C is found in plant foods such as citrus fruits, other fruits, and green leafy vegetables. It is considered an essential vitamin because humans don’t produce their own. Theoretically, we should get it easily in a balanced diet, yet there may be times we are deficient due to low intake or increased use in the body.
People who are ill are one of the primary populations in which vitamin C has been studied. Ill patients have an increased need for antioxidants because they have higher levels of inflammation, thus more increased intra- and extra-cellular reactive oxygen species. Normally, the body has a balance of both oxidative and reduced species, but during illness there is a pathological amount of ROS, which can damage DNA.
Adequate ascorbate levels are greater than or equal to 50 μmol/L plasma ascorbate concentration (vitamin C levels) (Carr et al., 2016). Hypovitaminosis C is defined as less than 23 μmol/L plasma ascorbate concentration in a study about critically ill patients and vitamin C deficiency (Carr et al., 2017). Hospitalized patients, for a variety of reasons such as viral illness, cancer, or various surgeries, have been found to have lower plasma vitamin C levels. A study of Scottish acute respiratory infection patients showed 35% had less than 11μmol/L vitamin C plasma levels (Hunt et al., 1994). A study of cancer hospice patients reported 30% of patients had less than 11μmol/L vitamin C plasma levels (Mayland et al., 2005). Another study in Paris found 44% of hospitalized patients had less than 6μmol/L (Teixeira et al., 2001). An Australian study of surgical patients found 21% had less than 11μmol/L vitamin C plasma levels (Ravindran et al., 2018).
The pattern of low vitamin C levels in patients seems to be common among infections, sepsis, surgery, trauma, burns, and stress which is reasonable considering the theory of increased metabolism in these conditions. This is important because this data shows ICU patients are still low in vitamin C despite receiving standard ICU enteral and parenteral (oral and IV) nutrition (Carr et al., 2017). This means the dosage of vitamin C would likely need to be increased for patients in these conditions compared to healthy people (Hemilä and Chalker, 2013).
The origin of exploring larger doses
Vitamin C has been delivered intravenously for decades, and in the last 20 years research has come a long way to determine safety, dosages, administration, and interactions.
Vitamin C has had some controversy over the years, but much of the stigma can be explained by different research design and administration routes.
In the 1970s, researchers Cameron and Pauling had compelling evidence for the use of supplemental intravenous vitamin C in terminal cancer patients with an oral dosage given afterward (Cameron and Pauling [1976, 1978]). They showed significant improvement in survival rates of those given the vitamin C. This included but was not limited to increased mean survival times of 300 days compared to the control group not treated with vitamin C.
Mayo Clinic did not have the same results when they tried to reproduce the findings in two follow-up studies in 1979 and 1985 (Creagan et al., 1979; Moertel et al., 1985), but they only used oral dosing. Because of the Mayo Clinic trials, medical vitamin C use became “alternative and complementary,” and some to this day say the Mayo trials disproved the originals, not discussing the vastly different study designs.
Controversy born out of comparing oranges to apples
The difference in findings was identified by Mark Levine’s research in the 1990s (Levine et al., 1996). He explained that Cameron and Pauling used intravenous and oral dosing, whereas the Mayo Clinic only studied oral dosing, and the pharmacokinetics are different. That would be like comparing oral Benadryl (diphenhydramine) to intravenous, or oral steroids to injected ones; they do not produce the same results.
We know through the pharmacokinetic research on vitamin C that in order to absorb it in the intestines, we need the sodium-dependent vitamin C transporter-1 (SVCT1) (Savini et al., 2008).
When we administer a medication by IV dosing, we bypass the gut. The SVCT1 transporter is not needed or used when vitamin C is given by IV (IVC), and the IV dosing can result in higher plasma levels of vitamin C because it doesn’t go through the GI tract (Carr and Cook, 2018).
With oral dosages of vitamins, they are also subject to food pairing, enzyme availability, stomach acid levels, and intestinal permeability. With oral vitamin C intake, we don’t see greater than 200μmol/L, but IVC can give plasma concentrations of 20mmol/L (Padayatty et al., 2004). Even if that’s a peak plasma concentration, that’s a 100x difference!
This isn’t the only time the evidence for vitamin C has been misconstrued. There was a famous trial in 1975 by Karlowski et al. that explored vitamin C and the common cold. The paper found a 17% decrease in the common cold in those who took vitamin C but concluded that “the effects demonstrated might be explained equally well by a break in the double blind.” This has since been cited “evidence” that vitamin C is useless in disease prevention. But in 1996 the findings were found to be incorrectly analyzed. The author showed that the placebo effect did not explain — and was inconsistent with — the results of the 1975 study (Hemilä,1996).
In fact, many studies since 1975 that explored vitamin C supplementation had design flaws that biased them against showing potential benefits. A 2013 article titled “Myths, Artifacts, and Fatal Flaws: Identifying Limitations and Opportunities in Vitamin C Research” discussed how these studies often failed to establish vitamin C levels or status at baseline so there was no proper benefit comparison. Another issue was that study enrollees were often health-conscious subjects with better-than-average diets and body weights. This means the “statistical power” of the studies were decreased. Many studies on vitamin C also didn’t account for the inclusion or exclusion of participants who smoked, drank alcohol, had high BMIs, had chronic aspirin use, or had low socioeconomic status — all factors associated with lower vitamin C status. All these factors decrease the ability of a randomized and controlled study to show improved health benefits with vitamin C supplementation (Michels and Frei, 2013).
Safety: avoid or lower dose in kidney problems and a genetic disease
Over the decades that vitamin C has been used intravenously, very few side effects have been seen. In nearly 1,000 patients studied, only 1% had side effects which included fatigue, lethargy, change in mental status, and vein irritation (Padayatty et al., 2010). Vitamin C metabolism can also break down in small percentages to calcium oxalate, so those prone to kidney stones are at a higher risk of side effects (Carr and Cook, 2018).
One of the main studies that demonstrated this administered the intravenous treatment continuously for two weeks (Riordan et al., 2005). Continuous dosing would only be used in a hospital setting like an ICU and isn’t a common usage of the treatment. In other studies that showed kidney dysfunction following IVC administration, all those who exhibited problems had existing renal dysfunction (Carr and Cook, 2018). This means that patients with kidney dysfunction should not receive high dosages of IVC. Another study found that kidney disease patients could be given 1.5g of IVC per kg of body weight with less than 0.5% conversion into oxalic acid, the substance that forms calcium oxalate crystals in kidney stones (Robitaille et al., 2009).
The other major risk factor for high-dose vitamin C infusions, like many other medications, is a glucose-6-phosphate dehydrogenase (G6PD) deficiency. In those with a G6PD deficiency, when many medications are given, including IVC, a hemolytic anemia can occur — which results in the damaging of red blood cells. This was seen when G6PD patients were given 80g of IVC (Rees et al., 1993). Follow-up case studies, pharmacokinetic data, and research has shown 10g or less of IVC given to G6PD patients is safe because this is not an oxidative dosage where in vivo hydrogen peroxide is created (Carr and Cook, 2018). G6PD deficiency occurs in about 400 million people worldwide and is prevalent among Kurdish Jews (60-70%), Nigerians (22%), Sardinians (4-35%), Thais (17%), and African Americans (11-12%) (Glader, 2020).
| Medicines and other substances likely to be UNSAFE in moderate to severe G6PD deficiency* [1-3] |
| Medications |
| Chlorpropamide |
| Dabrafenib |
| Dapsone (diaminodiphenyl sulfone) |
| Methylene blue (methylthioninium chloride) ¶ |
| Nitrofurantoin, nifuratel, and nitrofurazone (nitrofural) Δ |
| Phenazopyridine (pyridium) |
| Primaquine and tafenoquine |
| Rasburicase and pegloticase |
(Glader, 2020)
For this reason this treatment needs to be administered by a healthcare provider who understands physiology, biochemistry, and clinical data. You need to be properly screened to ensure you are a good candidate to receive the higher dosage treatments. There are documented benefits of lower doses such as 10g (or less) being administered intravenously. These are considered non-oxidative dosages that are safe for those with the G6PD trait, such as have been shown in quality-of-life (QOL) studies in cancer patients.
What does it do? Depends on the dose.
As discussed above, there are documented dose-dependent effects of vitamin C. Vitamin C itself is an antioxidant because it donates electrons. Vitamin C can be given in antioxidant dosages and pro-oxidant dosages. There is no standardization around the terms “low dose” and “high dose” vitamin C, so to avoid confusion many refer to it as antioxidant vs pro-oxidant. Ten grams or less is considered a non-oxidative or antioxidant dosage. Studies in the oncology field have found antioxidant dosing can be used to decrease fatigue, pain, nausea, vomiting, appetite loss and insomnia (Yeom et al., 2007). In fact the evidence shows it can increase overall health and functioning in these patients (Takahashi et al., 2012; Stephenson et al., 2013).
But when given at high dosages, such as over 10g, there is in vitro and in vivo research which shows that vitamin C acts differently (Carr and Cook, 2018). It can reduce metal ions, and the reduced transition metal ions can then generate H202 and cause oxidative stress (Carr and Frei, 1999). One of the main reasons vitamin C is used intravenously at high doses is for the pro-oxidant activity of generating hydrogen peroxide (H202).
Some studies even show that the addition of vitamin C causes different cytotoxicity (cell killing) in different cancer cell lines due to the generation of H202 (Chen et al., 2005, 2008). There are more mechanisms being studied inside cancer and cytotoxicity in animal and human studies around enzyme cofactor activities (Carr and Cook, 2018). These mechanisms are still under a lot of research and review, but it is clear there are vitamin-dependent anti-tumor mechanisms occurring in ongoing research that may be beneficial as adjunctive oncology therapies when the data becomes more clear.
Infection and fatigue benefits
There are many other reasons to explore and use vitamin C orally and intravenously, including as an antioxidant and for its anti-inflammatory properties. Vitamin C acts as an antioxidant both within cells and surrounding them in the plasma as it can “scavenge reactive oxygen species,” which protects cells from oxidative damage (Carr and Cook, 2018). One study even found that, at a low dosage of vitamin C given intravenously, healthy patients showed “decreased lipid oxidation biomarkers” (Muhlhofer et al., 2004).
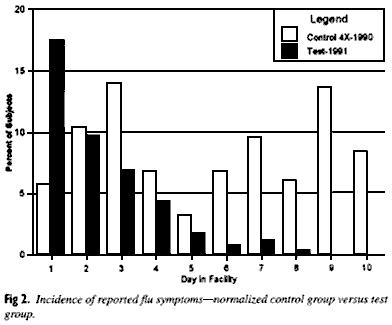
We also know through research that both oral and intravenous vitamin C have an effect on infections in the body. In 1999 a controlled, peer-reviewed study looked at the basic effect of high-dose vitamin C in the prevention and relief of virus-induced respiratory infections in 252 young adult students (with 463 control students). The control group received pain relievers and oral decongestants. The oral dosages of vitamin C in the test group were high at 1000mg hourly for 6 hours, then 1000mg three times daily. This is much higher than USDA says can be absorbed, with the US recommended daily allowance being 75mg for adult men and 70mg for adult women.
Many skeptics state the assumption that water-soluble vitamins like vitamin C taken in excess get passed into the urine so taking large doses are pointless. But the study found that those who received the high dose of vitamin C had symptom reduction of 85% compared to the control group. This showed that high doses of vitamin C given before or after cold/flu symptoms relieved and prevented symptoms (Gorton & Jarvis, 1999).
A review article titled “Vitamin C may affect lung infections,” written by two researchers in 2007, evaluated the effect of vitamin C on lung infections. They reviewed the likely mechanisms against infection before discussing the five controlled trials. One basic mechanism they identify is the antioxidant effect: “In the immune system, the major role of vitamin C seems to be as a physiological antioxidant, protecting host cells against oxidative stress caused by infections.” (Hemilä and Louhiala, 2007). They also discuss that, because of where vitamin C is found in high concentrations in the body, like in certain immune cells called phagocytes and lymphocytes compared to low amounts in plasma, it is likely playing a role in these immune cells’ functions (Hemilä and Louhiala, 2007). They also cite previous studies showing that vitamin C increases lymphocyte white blood cells and decreases replication of viruses (Hemilä, 2006), as well as animal research showing increased resistance against viral and bacterial infection when given vitamin C.
“Vitamin C may affect lung infections” also brings up compelling reasons for studying vitamin C specifically in pneumonia infections. Pneumonia leads to reduced vitamin C levels as measured in leukocyte immune cells, plasma and urine (Hemilä, 2006). Pneumonia was tied to scurvy in early literature about the disease (Hemilä and Louhiala, 2007). Scurvy, a major disease in the early 1900s, particularly among sailors who didn’t have access to fresh produce, was cured and prevented by vitamin C (Thomas, 1997). In 1920 a pediatrician examined scurvy patient autopsies and found that pneumonia was one of the most common complications in scurvy (Hess, 1920). This led researchers in Germany and the United States during the 1930s to study vitamin C and pneumonia directly. One of these studies during World War II was placebo-controlled, randomized, and double-blinded and found an 80% or more reduction in pneumonia when subjects were given vitamin C, which was statistically significant (Hemilä and Louhiala, 2007).
“Vitamin C may affect lung infections” explores the five modern controlled studies about vitamin C supplementation and pneumonia. They describe three trials that looked at prevention of pneumonia and two on treatment of pneumonia. Each study reviewed found “a statistically significant benefit of vitamin C supplementation on at least one clinically relevant outcome” (Hemilä and Louhiala, 2007). These authors were published in the Cochrane Library for a review on “Vitamin C for preventing and treating pneumonia,” six years later. The review evaluated five studies about vitamin C and pneumonia. The three prevention trials included were reviewed, and each had a statistically significant reduction in pneumonia incidence in the vitamin C groups. Vitamin C was not found to have any adverse effects in the five reviewed trials (Hemilä and Louhiala, 2013).
Vitamin C and the prevention and treatment of the common cold has mixed research. A randomized and controlled five-year study in Japan found that vitamin C supplementation reduced the frequency of the common cold but not the duration (Sasazuki et al., 2006). A different review article found that vitamin C, when taken regularly, did decrease the duration of a cold. This paper cited evidence that another study found vitamin C given to physically active people decreased cold incidence by half but didn’t have the same effect in the rest of the population (Hemilä, 2017). This author has pointed out that a reason for mixed and negative results for vitamin C and prevention of colds can be too low of dosing the vitamin.
The 2013 Cochrane Review, “Vitamin C for preventing and treating the common cold,” evaluated thirty-one trials that looked at regular vitamin C intake and found duration and severity of colds were reduced, while seven trials that evaluated therapeutic dosing found no reduction in duration or severity. The authors concluded that, “given the consistent effect of vitamin C on the duration and severity of colds in the regular supplementation studies, and the low cost and safety, it may be worthwhile for common cold patients to test … whether therapeutic vitamin C is beneficial for them” (Hemilä and Chalker, 2013).
Yet some studies found that the common cold was significantly reduced with vitamin C supplementation, such as four studies of British males decreasing colds by 30% (Hemilä, 1997) and those under acute physical stress (Hemilä, 1996). Studies found that vitamin C supplementation decreased the incidence of “chest colds” (the cold had cough or chest symptoms) (Elwood, 1976) and reduced the incidence of “throat colds” (Anderson, 1973). The “Vitamin C for preventing and treating pneumonia” review took this to mean that “vitamin C may have a greater effect on infections affecting the lower respiratory tract” (Hemilä and Louhiala, 2013).
A large, randomized, placebo-controlled, double-blinded study was published in the British Medical Journal of Military Health in March of 2020 to examine the association between vitamin C intake and the common cold in Korean army soldiers. The 1,444 participants were given either 6g of vitamin C per day or a placebo of no vitamin C. The vitamin C treatment group had an .80-fold lower risk of getting the common cold compared to the control group (Kim et al., 2020), indicating oral vitamin C was able to reduce viral infection risk.
There is also data for utilizing vitamin C against fatigue. A 2012 study published in The Nutrition Journal explored IV vitamin C in the use against fatigue in office workers. It was a double-blinded and randomized control trial. The treatment group was given 10g of vitamin C by IV, and the control group was given IV saline. They found IVC reduced fatigue at two hours and after one day, without significant differences in adverse effects between the two groups. The trial also reported the treatment group had lower oxidative stress compared to the control group (Suh et al., 2012).
Where does vitamin C land in the current disease environment?
There is currently no cure for the pandemic that is sweeping the globe. It is a virus, which means drug therapy is tricky. For most viruses we know of, there is a lack of effective and targeted drug therapies: symptomatic supportive care still resides as the main treatment. Pneumonia caused by viral infection is a serious condition that also has no cure and carries a very poor treatment success rate. Vitamin C is currently being studied in China as a potential, adjunctive intervention to support in combating this pandemic virus due to the antioxidant properties.
The phase 2 clinical trial began February 11th, 2020, and the estimated date of completion is September 30, 2020 (https://clinicaltrials.gov/ct2/show/NCT04264533). The theory is — and early clinical studies show — that vitamin C can prevent the process of specific immune cells surging during infection in the blood that leads to white blood cells accumulating in the lungs, destroying the air sac capillaries (tiny blood vessels) that allow us to exchange gases and breathe. Vitamin C can also prevent the vascular injury caused by white blood cell activation. This has been shown as a potential mechanism with vitamin C and other infections, such as influenza, so this research hopes to show a similar effect.
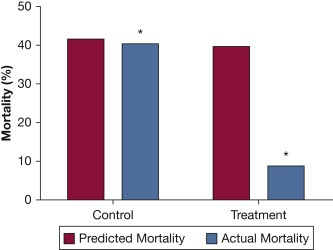
Many of these high-risk, viral-infected patients end up in the ICU for intensive treatment. There is established data that was published in a 2019 meta-analysis that showed vitamin C can shorten patients’ length of an ICU stay by 7.8%-8.6% and decrease the duration of mechanical ventilation by 18.2% (Hemilä and Chalker, 2019). In addition, a recent meta-analysis of eight trials found that mechanical ventilation of ill patients was decreased by an average of 14% when given vitamin C, and five trials that examined severely ill patients found ventilation was decreased by an average of 25% when given vitamin C (Hemilä and Chalker, 2020). There has also been significant reduction in mortality of ICU patients who were given vitamin C (Marik et al., 2016). As an ICU stay is highly costly to the hospital and patient — not to mention beds may be in short supply — even a moderate reduction in length of stay is worth exploring, especially when the treatment in question is relatively low in cost and can significantly impact mortality.
Patients with sepsis have also been evaluated for benefit with vitamin C use. A meta-analysis of three of these studies explored the data results and quality. The analysis demonstrated a “positive correlation between incorporating vitamin C in the treatment of sepsis and favorable patient outcomes, including better survival and shorter vasopressor use” (Li, 2018).
While the research for the use of vitamin C against viral pneumonia is still ongoing in China, there is established data to suggest prevention and management of oxidative stress with intravenous high-dose vitamin C treatments. The safety for the treatment has previously been established in data showing little to no side effects, and the potential to improve clinical outcomes is high. This may be why we are seeing U.S. hospitals finally add this to treatment regimens. In New York, under pulmonologist Andrew G. Weber, M.D., the Northwell Health facility ICUs are giving patients 1,500mg of intravenous vitamin C based on the previously cited study. He says, “patients who received the vitamin C did significantly better than those who did not get vitamin C” (Mongelli and Golding, 2020).
Let’s C the big picture
While some in the medical community continue to downplay the potential benefit of using both preventative and therapeutic vitamin C, studies continue to show many positive outcomes with limited negative side effects in a variety of conditions affecting a large population. Vitamin C is water soluble and is not at risk of overdosing, is not stored in the body, and has been shown to be low in ill patients; thus, supplementation has high potential for benefit with low risk. Medical practitioners in hospitals and clinics should stay open-minded to the low-cost, low-risk treatment option widely available for patients and consider adding vitamin C to treatment regimens if indicated. There is always room for ongoing research in treatment modalities that continue to show benefit in the medical literature, especially to explore dosages and how they can be refined for guidance of treatment.
Sources
Anderson TW, Reid DBW, Beaton GH. Vitamin C and the common cold. Canadian Medical Association Journal.1973;108(2):133.
Cameron, E., and Campbell, A. The orthomolecular treatment of cancer. II. Clinical trial of high-dose ascorbic acid supplements in advanced human cancer. Chem. Biol, Interact. 9. 1974;285–315.
Cameron, E., and Pauling, L.. Supplemental ascorbate in the supportive treatment of cancer: prolongation of survival times in terminal human cancer. Proc. Natl. Acad. Sci. U.S.A.1976;73 3685–3689.
Cameron, E., and Pauling, L. Supplemental ascorbate in the supportive treatment of cancer: reevaluation of prolongation of survival times in terminal human cancer. Proc. Natl. Acad. Sci. U.S.A.1978;75,4538–4542.
Carr, A. C., & Cook, J. Intravenous Vitamin C for Cancer Therapy – Identifying the Current Gaps in Our Knowledge. Frontiers in physiology. 2018;9:1182.
Carr, A., and Frei, B.. Does vitamin C act as a pro-oxidant under physiological conditions? FASEB J. 1999;13,1007–1024.
Carr, A.C.; Pullar, J.M.; Bozonet, S.M.; Vissers, M.C.M. Marginal Ascorbate Status (Hypovitaminosis C) Results in an Attenuated Response to Vitamin C Supplementation. Nutrients. 2016;8, 341.
Carr, A.C., Rosengrave, P.C., Bayer, S. et al. Hypovitaminosis C and vitamin C deficiency in critically ill patients despite recommended enteral and parenteral intakes.Crit Care. 2017;21, 300.
Chen, Q., Espey, M. G. et al.. Pharmacologic ascorbic acid concentrations selectively kill cancer cells: action as a pro-drug to deliver hydrogen peroxide to tissues. Proc. Natl. Acad. Sci. U.S.A. 2005;102,13604–13609.
Chen, Q., Espey, M. G., Sun, A. Y., Pooput, C., Kirk, K. L., Krishna, M. C., et al.. Pharmacologic doses of ascorbate act as a prooxidant and decrease growth of aggressive tumor xenografts in mice. Proc. Natl. Acad. Sci. U.S.A. 2008;105,11105–11109.
Creagan, E. T., Moertel, C. G., O’Fallon, J. R., Schutt, A. J., O’Connell, M. J., Rubin, J., et al. . Failure of high-dose vitamin C (ascorbic acid) therapy to benefit patients with advanced cancer. A controlled trial. N. Engl. J. Med. 1979;301,687–690.
Glader, B. Diagnosis and management of glucose-6-phosphate dehydrogenase (G6PD) deficiency. In: UpToDate, Post, DM (Ed), UpToDate, 2020.
Elwood PC, Lee HP, Leger AS, Baird IM, Howard AN. A randomized controlled trial of vitamin C in the prevention and amelioration of the common cold. British Journal of Preventive and Social Medicine 1976;30(3):193-6.
Gorton HC, & Jarvis K. The effectiveness of vitamin C in preventing and relieving the symptoms of virus-induced respiratory infections. Journal of Manipulative & Physiological Therapeutics. 1999;22(8), 530–533.
Hemilä H. Do vitamins C and E affect respiratory infections? [Dissertation]. Helsinki, Finland: University of Helsinki, 2006;1-9,58-67,101-4.
Hemilä H. Vitamin C and common cold incidence: a review of studies with subjects under heavy physical stress. International Journal of Sports Medicine.1996;17(5):379-83.
Hemilä H. Vitamin C and Infections. Nutrients. 2017; 9(4):339.
Hemilä H. Vitamin C intake and susceptibility to the common cold [comments in: 1997;78(5):857-66]. British Journal of Nutrition. 1997;77(1):59-72.
Hemilä, H.; Chalker, E. Vitamin C Can Shorten the Length of Stay in the ICU: A Meta-Analysis. Nutrients 2019;11, 708.
Hemilä, H., Chalker, E. Vitamin C may reduce the duration of mechanical ventilation in critically ill patients: a meta-regression analysis. j intensive care 8, 15 (2020).
Hemilä H, Chalker E. Vitamin C for preventing and treating the common cold. Cochrane Database of Systematic Reviews. 2013; Issue 1. Art. No.: CD000980.
Hemilä H, Louhiala P. Vitamin C for preventing and treating pneumonia. Cochrane Database Syst Rev 2013;(8),8.
Hemilä, H., & Louhiala, P. . Vitamin C may affect lung infections. Journal of the Royal Society of Medicine. 2007;100(11),495–498.
Hess AF. Scurvy: Past and Present. Philadelphia, PA: Lippincott. 1920:88, 99.
Hunt, C.; Chakravorty, N.K.; Annan, G.; Habibzadeh, N.; Schorah, C.J. The clinical effects of vitamin C supplementation in elderly hospitalised patients with acute respiratory infections. Int. J. Vitam. Nutr. Res.1994;64,212–219.
Karlowski TR, Chalmers TC, Frenkel LD, et al. Ascorbic acid for the common cold: a prophylactic and therapeutic trial. JAMA.1975;231(10):1038–1042.
Kim TK, Lim HR, Byun JSVitamin C supplementation reduces the odds of developing a common cold in Republic of Korea Army recruits: randomised controlled trial. BMJ Mil Health Published Online First: 05 March 2020.
Li, J. Evidence is stronger than you think: a meta-analysis of vitamin C use in patients with sepsis. Crit Care.2018;22,258.
Mayland, C.R.; Bennett, M.I.; Allan, K. Vitamin C deficiency in cancer patients. Palliat. Med. 2005;19,17–20.
Michels, A.J.; Frei, B. Myths, Artifacts, and Fatal Flaws: Identifying Limitations and Opportunities in Vitamin C Research. Nutrients 2013;5, 5161-5192.
Mongelli, L., & Golding, B. New York hospitals treating coronavirus patients with vitamin C. The New York Post March 24, 2020.
Muhlhofer, A., Mrosek, S., Schlegel, B., Trommer, W., Rozario, F., Bohles, H., et al. High-dose intravenous vitamin C is not associated with an increase of pro-oxidative biomarkers. Eur. J. Clin. Nutr. 2004;58, 1151–1158.
Nabzdyk, C. S., & Bittner, E. A. Vitamin C in the critically ill – indications and controversies. World journal of critical care medicine, 2018;7(5), 52–61.
Padayatty, S. J., Sun, A. Y., Chen, Q., Espey, M. G., Drisko, J., and Levine, M. Vitamin C: intravenous use by complementary and alternative medicine practitioners and adverse effects. PLoS One. 2010; 5:e11414.
Padayatty, S. J., Sun, H., Wang, Y., Riordan, H. D., Hewitt, S. M., Katz, A., et al. Vitamin C pharmacokinetics: implications for oral and intravenous use. Ann. Int. Med. 2004;140, 533–537.
P.E. Marik, V. Khangoora, R. Rivera, M.H. Hooper, J. Catravas. Hydrocortisone, vitamin C, and thiamine for the treatment of severe sepsis and septic shock: a retrospective before-after study Chest, 151. 2017; 1229-1238.
Ravindran, P.; Wiltshire, S.; Das, K.; Wilson, R.B. Vitamin C deficiency in an Australian cohort of metropolitan surgical patients. Pathology 2018;50,654–658.
Rees, D. C., Kelsey, H., and Richards, J. D. Acute haemolysis induced by high dose ascorbic acid in glucose-6-phosphate dehydrogenase deficiency. BMJ.1993;306,841–842.
Riordan, H. D., Casciari, J. J., Gonzalez, M. J., Riordan, N. H., Miranda-Massari, J. R., Taylor, P., et al. A pilot clinical study of continuous intravenous ascorbate in terminal cancer patients. PR Health Sci. J. 2005;24,269–276.
Robitaille, L., Mamer, O. A., Miller, W. H. Jr., Levine, M., Assouline, S., Melnychuk, D., et al. Oxalic acid excretion after intravenous ascorbic acid administration. Metabolism 2009;58, 263–269.
Savini, I., Rossi, A., Pierro, C., Avigliano, L., and Catani, M. V. SVCT1 and SVCT2: key proteins for vitamin C uptake. Amino Acids 2008;34, 347–355.
Sasazuki, S., Sasaki, S., Tsubono, Y., Okubo, S., Hayashi, M., & Tsugane, S. Effect of vitamin C on common cold: Randomized controlled trial. European Journal of Clinical Nutrition, 2006;60(1), 9-17.
Stephenson, C. M., Levin, R. D., Spector, T., and Lis, C. G. Phase I clinical trial to evaluate the safety, tolerability, and pharmacokinetics of high-dose intravenous ascorbic acid in patients with advanced cancer. Cancer Chemother. Pharmacol. 2013;72,139–146.
Suh, S., Bae, W. K., Ahn, H., Choi, S., Jung, G., & Yeom, C. H. Intravenous vitamin C administration reduces fatigue in office workers: A double-blind randomized controlled trial. Nutrition Journal, 2012;11, 7.
Takahashi, H., Mizuno, H., and Yanagisawa, A. High-dose intravenous vitamin C improves quality of life in cancer patients. Personal. Med. Universe. 2012;2, 49–53.
Teixeira, A.; Carrie, A.S.; Genereau, T.; Herson, S.; Cherin, P. Vitamin C deficiency in elderly hospitalized patients. Am. J. Med. 2001;111, 502.
Thomas DP. Sailors, scurvy and science. J R Soc Med 1997;90:50-54.
Yeom, C. H., Jung, G. C., and Song, K. J.. Changes of terminal cancer patients’ health-related quality of life after high dose vitamin C administration. J. Korean Med. Sci. 2007; 22, 7–11.